





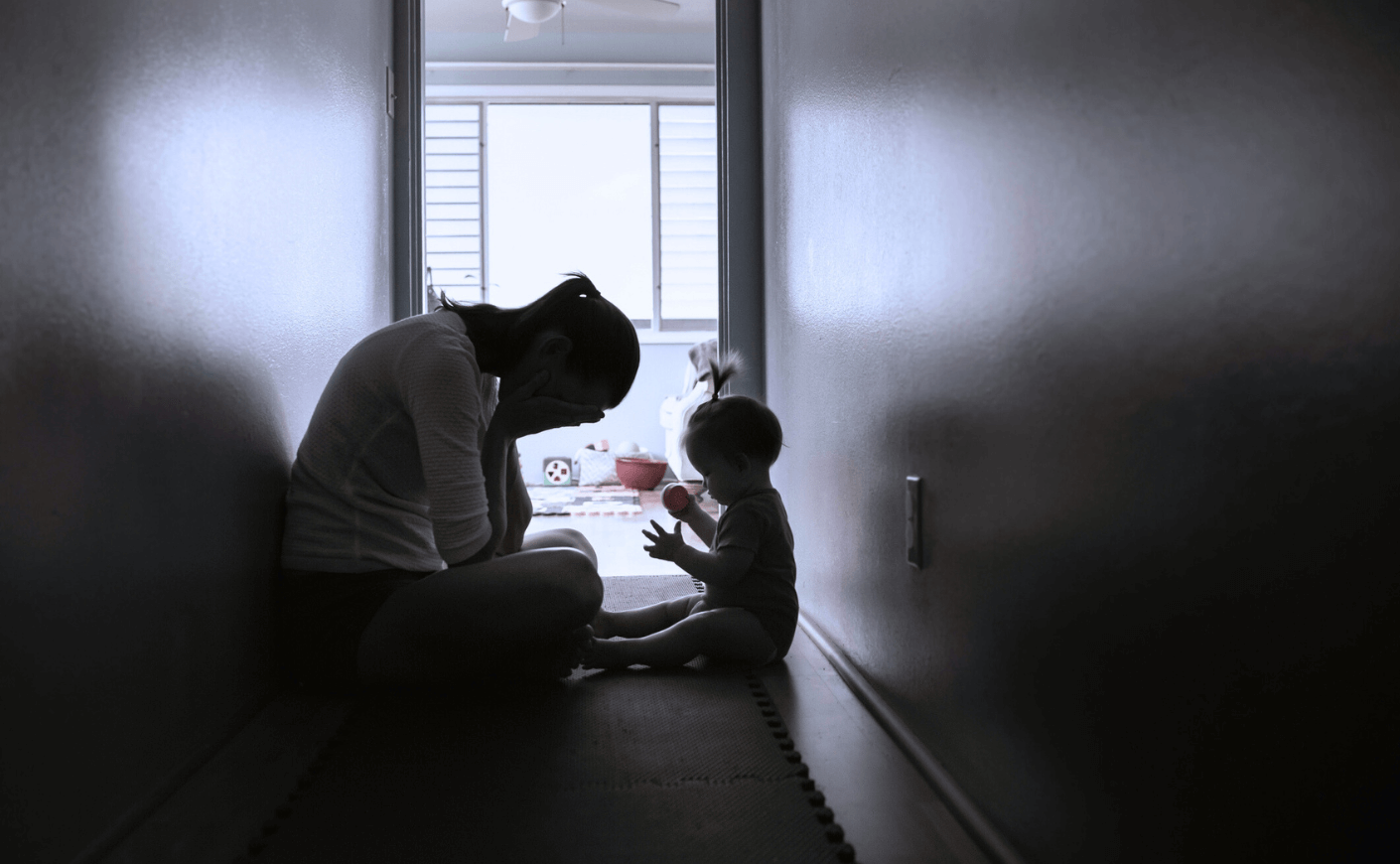
I hadn’t slept for five days when I dropped to my knees and curled up in the fetal position on my newborn son’s nursery room carpet. Maybe on the floor, I’d feel safe.
Max was finally home from five weeks in the NICU. You’d think now I could finally relax. Instead, the heaviest kind of depression held me down. But how could this be happening to me? How could I — a second-time mom — be glued to my son’s floor? Heaping shame upon shame, I was also a clinical psychologist specializing in treating postpartum. Just a month ago, I was sitting in a chair treating my patients. So, how was I now the one who needed help?
To add context to my personal catastrophe, it was March of 2020 and the COVID pandemic was blooming, sending people to hospitals and killing them. My husband, a physician, was there on the front lines. Our newborn was in a hospital nearby.
But now Max was finally home with his mom, dad, and three-year-old sister, all needing protection from the unknown deadly respiratory disease circulating outside our front door, and I had to be the one doing the protecting. The irony of Max being born into a world struggling to breathe, while he himself needed breathing support, was not lost on me.
Hypervigilance consumed me. Strangely enough, my pregnancy and childbirth had also been ferocious and terrifying, but not nearly as frightening as keeping my family safe. I’d spent nine months vomiting, with severe and relentless hyperemesis gravidarum (HG). That condition, for those lucky enough not to know about it, is debilitating nausea and vomiting during pregnancy. The birth was quite a follow-up act: Max was pulled from me in a middle-of-the-night C-section.
That rock-bottom day in my son’s nursery, I somehow peeled myself off the carpet and called my doctor. My death grip on my phone loosened when my psychiatrist prescribed medication immediately, and reassured me that my postpartum was treatable. Within nine days, I felt better.
Mothers are used to fighting uphill battles.
I’m certainly not alone. Postpartum depression rates have soared since COVID — it’s now estimated to impact 1 in 3 mothers. And birth trauma occurs in 13 percent of all deliveries, though both those figures are likely gross underestimates, given the reluctance and shame around reporting symptoms — nursing mothers are afraid to be medicated, in case any of those medications might negatively affect the baby. Effective postpartum treatments are available and new treatments are being tested, but there’s still a huge health disparity in which only 4 percent of total research funding goes to research on women’s health issues.
But mothers are used to fighting uphill battles.
When a baby is born, so is its mother in a sense, given that childbirth is an experience that overhauls a woman’s psyche. In fact, Yale researchers now deem matrescence as the neurodevelopmental phase of profound neuroplasticity, identity, relationship, and emotional changes. While the brainpower boosts can cause anxiety (see above), they can also aid with both triggering and managing distress: cue the mom guilt, mom shame, and mom rage.
During matrescence, the brain changes rapidly, fine-tuning and priming itself for new learning. At the same time, the brain sheds useless neural networks known as synaptic pruning. Basically, the process is like Marie Kondo’ing for your mind, equipping moms with an optimal brain for caregiving.
Moms have postpartum superpowers, but sometimes all that kinetic brain activity can go haywire, and the result can be postpartum mental health disorders, as happened with me. Postpartum treatment rescued me from crisis, and then ordinary miracles kicked in: In only several short months after my postpartum crises, I found myself thriving amidst a global pandemic on our doorstep, experiencing newfound meaning, joy, and bursts of creativity. Feeling better than ever after experiencing the normative trauma of becoming a mother, coupled with global trauma, is what the field of positive psychology would call post-traumatic growth (PTG).
I wrote my book Rattled to share what I’ve learned through experience and research. In it, I describe how evidence-based postpartum mental health treatment can help mothers get to the other side of trauma by facilitating PTG. Postpartum treatment for mental illnesses can go that much further because mothers are primed for new learning. Moms in the transformative phase of matrescence are motivated to feel better so that they can take better care of their babies and break maladaptive intergenerational cycles. Let’s utilize the cognitive boosts and self-directed neuroplasticity to harness changes to women’s advantage.
What we need now is change: Rattled is my call to action to dismantle the barriers to maternal well-being and usher in a new era of empowerment and resilience for mothers everywhere. We need evidence-based postpartum mental health treatment to be the standard of care for all women. Companies can invest in maternity leave proactively so that mothers can pay for treatment and instrumental support. In this way, matrescence can resemble more of an employee development program — with enhanced skills, brain power, and assets to employers — versus a mental health crisis. And together, we can rewrite the narrative of motherhood, transforming trauma into triumph and despair into hope. The journey may be arduous, but the destination is nothing short of revolutionary.
Nicole Amoyal Pensak, Ph.D., is a Harvard and Yale-trained clinical psychologist, author of Rattled: How to Calm New Mom Anxiety with the Power of the Postpartum Brain, and a researcher specializing in treating anxiety, OCD, and depression, and certified in postpartum mental health. Dr. Pensak provides evidence-based treatment and serves on the Expert Review Board for Parents magazine.