






Until recently, the most effective new obesity medications, including semaglutide (Wegovy) and tirzepatide (Zepbound), were available only as injectables. That limited access; some patients are afraid of needles, can't guarantee refrigeration due to frequent travel, or simply prefer a pill.
That's all about to change. Oral options are arriving, which means accessibility will stretch much wider. So far, Novo Nordisk’s oral semaglutide and Lilly’s orforglipron are available. (Tirzepatide has not been tested or FDA-approved in pill form, but that hasn't stopped some companies from trying to sell it.)
Despite the inconvenience of an injection, use of these medications has become widespread. Like the original formula, GLP-1 pills are intended for adults with obesity, or adults with overweight and at least one weight-related medical condition — they aren't meant to achieve cosmetic goals. They are powerful medications for chronic disease and require medical care, follow-up, and realistic expectations. Unfortunately, the population of patients misusing these medications is only going to increase as they become easier to ingest.
Here's what else to expect from the GLP-1 pills, including their efficacy and availability.
How do GLP-1 pills work?
GLP-1 stands for glucagon-like peptide-1, a nutrient-stimulated hormone released by the intestine after eating. GLP-1 medications act on receptors in the brain and gut to increase feelings of fullness, decrease cravings, slow stomach emptying, and improve blood sugar regulation.
Many patients describe feeling full sooner, needing smaller portions, or having quieter “food noise” — persistent, intrusive thoughts about food reported by many patients with obesity. That can be incredibly meaningful, especially for people who have spent years being told, directly or indirectly, that weight is simply a matter of willpower. These medications are another reminder that obesity is a complex chronic disease influenced by biology, genetics, medications, sleep, stress, food environments, and social factors.
But they are not magic, and they are not short-term medications. Like treatments for high blood pressure or diabetes, they work best when patients receive ongoing care and support. Many people regain weight when they stop taking them, which is why patients should think carefully about whether they are ready for long-term treatment, at least until we have better evidence on how to maintain weight loss after stopping medication or treatments that more durably change the course of obesity.
How is orforglipron (Foundayo) different from the semaglutide (Wegovy) pill?
Both semaglutide and orforglipron pills are taken by mouth once daily. Each starts at a low dose that can be increased every four weeks as tolerated and needed.
Semaglutide is a peptide that is poorly absorbed in the stomach (<1 percent reaches your blood), so it must be taken on an empty stomach in the morning, with no more than 4 ounces of water. Patients must then wait at least 30 minutes before eating, drinking, or taking other oral medications to improve absorption.
Orforglipron, on the other hand, is a small-molecule GLP-1 receptor agonist that is better absorbed. This means it can be taken without the same food and water restrictions as oral semaglutide and could be easier for busy people who can’t afford to wait 30 minutes before having breakfast.Besides convenience, other factors, such as side effects and efficacy, will help determine which medication is best for you.
How effective are the weight loss pills?
The Wegovy pill appears to produce weight loss in the same general range as injectable Wegovy. In a clinical trial, called OASIS 4, oral semaglutide 25 mg led to an average weight loss of about 13.6 percent over 68 weeks.
Orforglipron also produced significant but somewhat lower weight loss than oral semaglutide. In a clinical trial, the highest dose of orforglipron led to 11.2 percent weight loss at 72 weeks. But they have not been compared in head-to-head trials.
How does this compare with injectables? Injectable Wegovy produced an average weight loss of around 15 percent in major trials, while tirzepatide, sold as Zepbound for obesity, has produced around 20 percent or more weight loss depending on dose and population.
What are the side effects of oral GLP-1s?
The most common side effects for both medications are gastrointestinal: nausea, vomiting, diarrhea, constipation, reflux, and abdominal discomfort. These often happen during dose escalation and usually improve over time and with adequate support from a healthcare provider. Orforglipron may have higher rates of these side effects than oral semaglutide, and more people may discontinue orforglipron as a result. Orforglipron also is more likely to increase heart rate (by about 4 beats per minute).
There are also less common but important risks, including gallbladder disease, pancreatitis, dehydration from vomiting or diarrhea, worsening reflux or gastroparesis symptoms.
All weight loss leads to both fat and muscle loss, which can be a concern, especially in people who are already frail. Maintaining adequate nutrition and exercise, including appropriate protein intake and resistance training, can help prevent loss of strength in most patients.
How much do GLP-1 pills cost, and will they be cheaper than injections?
Cost has been one of the biggest barriers to treatment, with many patients unable to access these medications because insurance coverage is limited and out-of-pocket prices remain high.
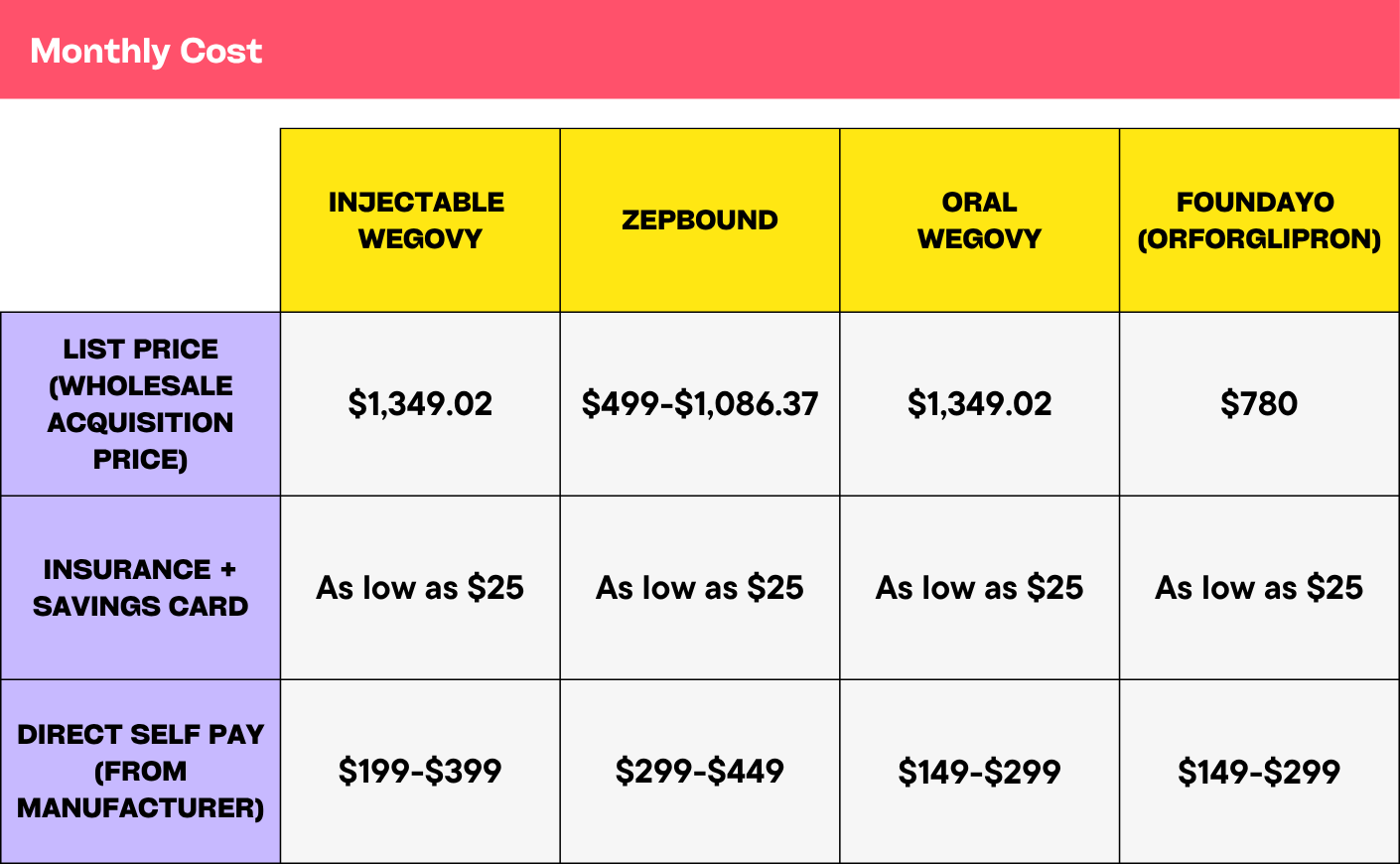
Pills are currently a little cheaper than injections, but the pricing is still evolving.
Competition from oral medications may eventually help lower prices. New Medicare and Medicaid access programs could also make a difference, but the details will matter: eligibility, prior authorization, which drugs are included, and whether state Medicaid programs participate. Below is a chart breaking down GLP-1 pill pricing.
What are the potential risks of the new pills?
While I’m excited that patients may soon have more options, enthusiasm should not blind us to the risks. Oral medications may feel easier to obtain, easier to hide, and easier to misuse.
- Medication without support: These drugs work best with counseling around nutrition, physical activity, strength training, side effects, and long-term adherence. Without that support, patients may lose muscle, struggle with nutrition, stop too soon, or feel abandoned when side effects occur or weight returns.
- Cosmetic weight loss and “longevity”: These medications are being marketed to people who do not meet medical criteria, including those who simply feel pressured to be thinner. We do not yet have evidence that they're safe for people without obesity, diabetes, and/or cardiometabolic disease. We also lack evidence that they extend lifespan in otherwise healthy people.
- Copycat products and inadequate oversight: We already have a troubling market of compounded products, “research” peptides, microdosing plans, longevity packages, and cosmetic weight-loss programs with inadequate medical supervision. Pills could make this marketplace even harder to navigate.
- Misuse and abuse: Pills may be easier to conceal, share, or overuse than injectables. That raises concerns for teenagers, young adults, people with eating disorders, and anyone buying medications from sketchy online sellers.
- Stigma: These medications should help us understand obesity as a chronic, biologically driven disease. Instead, they are too often folded back into diet culture, where thinness is treated as the goal.
Oral GLP-1 medications are an exciting advance. They may make effective obesity treatment easier, more acceptable, and eventually more affordable for many people.
But a pill is still a powerful medicine. These drugs should not be sold as cosmetic shortcuts, “longevity” hacks, or quick fixes. They should be used for the right medical reasons, with strong clinical support, and with a long-term plan focused on health, not thinness at any cost.
Melanie Jay, MD, MS, is a professor of medicine and population health at NYU Langone Health and a physician investigator specializing in obesity. Her research focuses on improving the treatment of obesity in medical settings and addressing weight stigma.